
Table of Contents
COPD
Chronic obstructive pulmonary disease (COPD) is a general term referring to a group of progressive disorders characterized by pulmonary ventilation impairment. In other words, you have COPD when you are unable to normally exchange air between your lungs and the ambient air (breathe). Most often, chronic obstructive pulmonary disease includes chronic bronchitis and emphysema. Asthma is also considered as a chronic obstructive pulmonary disease; however, its attack is temporary, unlike chronic bronchitis and emphysema of which symptoms are permanent and tend to get worse over time.
COPD is characterized by a slow and progressive narrowing or obstruction of the airways. The obstruction makes it difficult for you to breathe, and lead to occurrence of “annoying” symptoms such as shortness of breath and chronic cough. Without a proper treatment, COPD will make your life very miserable and can even kill you.
Fortunately, in developed countries like the United States, there are now effective treatments that can improve the life of patients living with chronic obstructive pulmonary disease.
 Incidence
Incidence

Although there is treatment to combat the disease, that does not prevent chronic obstructive pulmonary disease (COPD) from being a very common lung disease and one of the top 10 killers in the world. According to the World Health Organization (WHO), it is estimated that about 210 million people suffer from COPD worldwide, causing more than three million deaths in 2005, which corresponds to 5% of all deaths occurred worldwide that year. The worst is that this number may increase by over 30% in ten years if no formal actions are taken against tobacco smoke, the primary cause of chronic obstructive pulmonary disease.
COPD Causes and Risk Factors
COPD is a respiratory disease characterized by chronic inflammation of the lung tissue. Its development is mainly related to pollution or cigarette smoke entering the lungs, and causing destruction of the tissue in the large airways or the alveoli. The abnormal inflammatory response in the airways is called chronic bronchitis; emphysema occurs when the inflammation develops in the alveoli. In some cases, chronic obstructive pulmonary disease can be resulted from an asthmatic bronchitis.
Chronic bronchitis – Chronic bronchitis is a very common lung disease. It is characterized by inflammation of the lining of the lungs, which leads to excess production of secretions in the bronchial tree. The tunica mucosa of the bronchi (mucous membrane lining the bronchi structures) begins from the trachea and ramifies in the left and right lobes of the lungs. It is a thin membrane. When it is constantly irritated, it becomes swollen and reduced in diameter. The swelling of the bronchi and bronchioles, and excess mucus therein in the bronchial tubes cause a decrease or difficulty of breathing.
In general, you are diagnosed with chronic bronchitis if you produce phlegm (a sticky fluid secreted by the mucous membrane of the respiratory tract) almost daily for at least three months per year for at least two years. In addition to excessive secretions, chronic bronchitis is often associated with respiratory infections and shortness of breath.
Emphysema – this is a dilation or swelling of the alveoli of the lungs associated with destruction of their elastic wall (alveolar wall), making it difficult for them to completely empty at the expiration of the air they contain. The alveoli are part of the lungs where most of the gas exchange occurs: this is where the oxygen in the air enters the bloodstream, and the blood is freed from carbon dioxide. Any damage in the alveoli will cause a reduction or difficulty of gas exchange, which can lead to shortness of breath, cough and general malaise. In the genesis of emphysema, shortness of breath occurs during activities; however, as the disease worsens, shortness of breath may occur even at rest. Emphysema is often associated with chronic bronchitis.
Asthma – asthma is a lung disease of allergic nature, characterized by respiratory problems. In general, asthma is due to narrowing or excessive contraction of the bronchi. It is often associated with shortness of breath, wheezing and coughing. When you have asthma, your airways are much more responsive than normal to various stimuli: chemical, pollen, etc.
Risk Factors
A variety of risk factors are suspected in the development of asthma; the most common include:
Cigarette smoking – besides a variety of cancer, tobacco use (including second hand smoke) is the primary causative factor of COPD. It is estimated that nearly 90% of cases of chronic obstructive pulmonary disease in the U.S. are smoking related.
Age – age does not cause chronic obstructive pulmonary disease, however, the risk of chronic obstructive pulmonary disease increases with age. The disease tends to occur among people over 40.
Genetics – researchers theorize that there is a genetic predisposition to developing chronic obstructive pulmonary disease among certain individuals. The disease is more common in those who smoke and have parents who have COPD. Genetic disorder suspected is Alpha 1-antitrypsin, a genetic disease that is responsible for 2% of chronic obstructive pulmonary disease cases.
Being in a developing country – according to World Health Organization (WHO), nearly 90% of COPD deaths happen in developing countries where effective strategies for prevention and control of chronic obstructive pulmonary disease are not applied.
Chronic infection – frequent infections of the lower airways during childhood may lead to the development of chronic obstructive pulmonary disease.
Occupation – it is estimated that 15% of cases of chronic obstructive bronchopneumonia are of occupational origin. You are at greater risk of chronic obstructive pulmonary disease if you work in:
- coal mine
- hard rock mine
- tunnel
- concrete Industry
- rubber manufacturer
- leather
- public utilities
- textile
- Construction or other occupations that expose you to cigarette smoke, polluted air and various gases, dusts and fumes.
COPD Symptoms
At early stage, chronic obstructive pulmonary disease tends to be asymptomatic; the disease produces no symptoms, but continues its ravage in your lung tissue. Most of the times, when symptoms finally immerge, your lungs and airways are already damaged.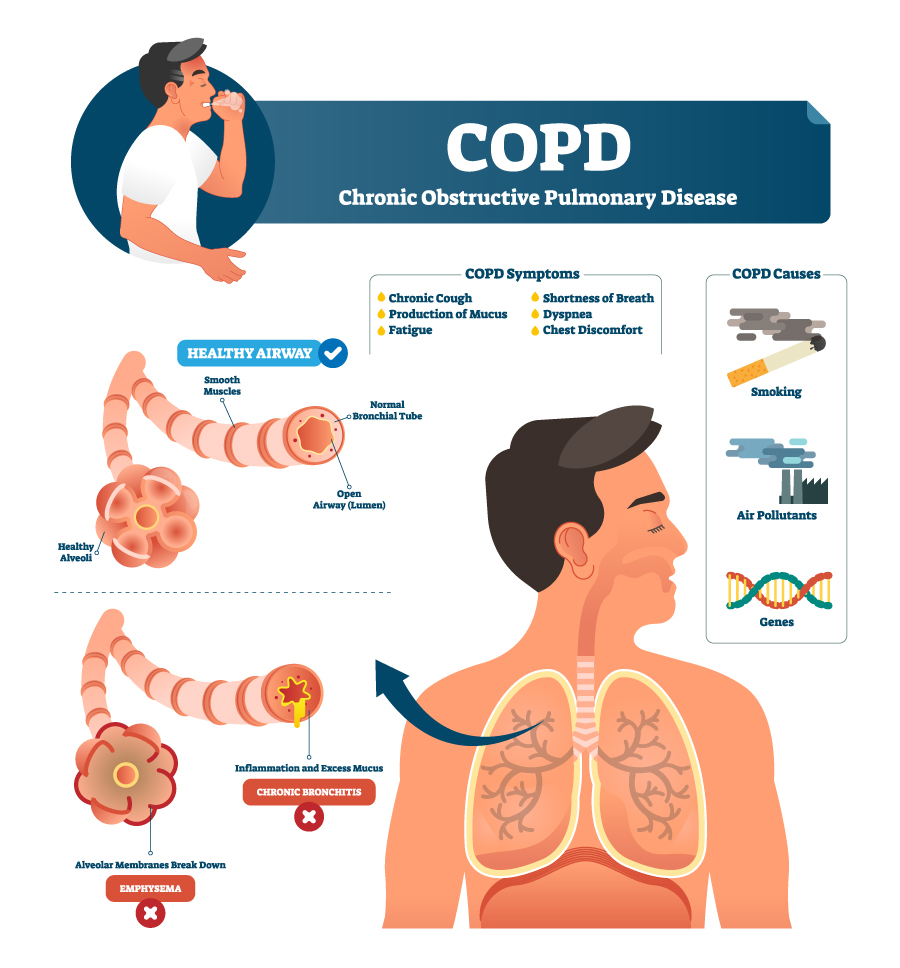
Knowing the symptoms of COPD is very important; it helps you to seek medical care before the disease severely damages your lungs and airways. Early detection of chronic obstructive pulmonary disease increases your chance of recovery or prevents complications. COPD symptoms include all the symptoms of chronic bronchitis, emphysema and asthma; however, the most common symptoms are chronic cough, breathlessness and abnormal sputum (mixture of saliva and mucus in the airways). These symptoms may be aggravated during daily life activities; for instance, climbing stairs or carrying a suitcase. As the disease worsens, you may also experience:
- Wheezing
- Shortness of breath
- chest tightness and pressure
- Chronic or frequent respiratory infections
- Persistent cough that produces yellowish sputum
- Persistent need to clear your throat, especially in the morning
- Fatigue during daily activities or during minor physical exercises.
Complications
The major complication of COPD is respiratory failure, the lungs and bronchial tubes become unable to function normally, which will eventually lead to a low level of oxygen and/or high level of carbon dioxide in the blood
Lack of oxygen can lead to bacterial or viral lung infection, which can lead to COPD exacerbation, abrupt and severe worsening of COPD symptoms. Respiratory failure may also evolve into an acute respiratory distress syndrome (a life threatening condition characterized by inflammation of the lungs, accumulation of fluid in the alveolar air sacs, and low blood oxygen) and private certain organs (brain, kidney, etc.) of the body of oxygen needed to function properly. If left untreated, this condition can cause death by asphyxiation.
Although rare, if you have chronic obstructive pulmonary disease, you are at higher risk of having lung cancer, depression, and heart disease, including heart attack. To prevent COPD complications, it is necessary to take your medications as recommended by your doctor or pharmacist, and see your health care provider if the symptoms worsen.
Diagnosis
The fact that symptoms appear only in a later stage of the disease, chronic obstructive pulmonary disease is often diagnosed late after the disease has already damaged the lungs. During the diagnosis, your doctor will do a clinical examination searching for signs of the disease. However, a normal clinical examination does not rule out COPD, other more specific tests will be performed to detect the disease.
Once you are diagnosed with COPD, it is extremely important to stop smoking if you are a smoker. Stopping smoking not only increases your chance of recovery but lower your chances of complications such as respiratory failure and lung cancer. In general, your doctor will perform some or all of the following exams:
Pulmonary function tests – Most of the times, these tests are done with a spirometer to detect various respiratory problems such as asthma and COPD. They are performed to examine respiratory function in order to have precise information on the type of respiratory disease in question and its severity. A pulmonary function testing not only allows your physician to discover a chronic obstructive pulmonary disease but also determine the impact it is already done in the lungs and airways.
During the exam, you will be asked to relax and comfortably install near the camera. Being in a position to easily breathe, the health care provider will ask you to do a few normal breaths before asking you to blow into a large tube connected to a spirometer. You need to inhale deeply and slowly and start blowing by a forced and rapid expiration to expel the maximum air possible from your lungs. Usually, the examination consists of three forced expirations of this type. It is preferable to not fill your stomach or smoke at least 5 hours before the examination.
Chest X-ray – this imaging technique is the basic examination to confirm emphysema or rule out other lung problems or heart failure that may present symptoms similar to those of COPD. A chest x-ray allows your physician to examine not only your lungs but also your trachea, bronchi, the two layers that surround the lung (pleura), heart and ribs.
Sputum examination – this exam helps your doctor to identify pathogens causing the lungs problems, and screen for malignant cells, if there is any.
Arterial blood gas analysis – this test include measuring the carbon dioxide pressure (pCO2), the pressure of oxygen (pO2) and the activity of hydrogen ion (or pH) in arterial blood. Analysis of blood gas is made from a sample of arterial blood taken from the wrist (radial puncture) by a syringe. The sample must be quickly transported to the laboratory – within 20 minutes – for examination. This procedure allows your doctor to measure the concentration of CO2 and oxygen saturation (SaO2) in your plasma.
Computerized tomography (CT) scan – a CT scan is a radiological diagnostic method consisting of penetration of X-rays in the body’s internal organs, and the use of a computer for analysis of the results. The CT scan of the chest allows your physician to explore your heart, lungs and arteries to detect certain pathologies related to chronic obstructive pulmonary disease.
COPD Treatment
 There is no cure for COPD; there are, however, treatments that can help you live a better life. Treatments aim to reduce symptoms and prevent bronchial infection. In addition, the treatments can help reduce damage to the heart muscle, prevent respiratory failure and other complications related to chronic obstructive pulmonary disease. Treatment should be started as early as possible; without treatment, COPD can develop into chronic respiratory failure and even death.
There is no cure for COPD; there are, however, treatments that can help you live a better life. Treatments aim to reduce symptoms and prevent bronchial infection. In addition, the treatments can help reduce damage to the heart muscle, prevent respiratory failure and other complications related to chronic obstructive pulmonary disease. Treatment should be started as early as possible; without treatment, COPD can develop into chronic respiratory failure and even death.
Also, it is extremely important to stop smoking if you are a smoker. If you live with smokers, you need avoid cigarette smoke – second hand smoke. Exposure to cigarette smoke and other pollutants in the air can not only aggravate the COPD symptoms but also reduce the therapeutic effects of the drugs.
Usually, COPD treatment includes medications, surgery and/or oxygen therapy:
Medications
Bronchodilators – Bronchodilators are drugs used to relax the muscles around the airways. They help to prevent bronchoconstriction (constriction of the airways in the lungs) or bronchospasm (sudden and abnormal contraction of the smooth muscle of the bronchi) in respiratory diseases such as asthma, emphysema and chronic bronchitis, three primarily related diseases of chronic obstructive pulmonary disease (COPD).
Anti-Inflammatory drugs – breathing difficulty you experience is due to inflammation of the airways. To help you breathe easier, your physician can recommend you to inhale corticosteroids or take corticosteroid pills. Although those drugs can improve the quality of your life, taking them for a prolonged time can damage vital tissues of your body and increase your risk of hypertension, cataracts and diabetes.
Antibiotics – to prevent or fight infections, which can aggravate the symptoms of COPD, your doctor may recommend you to take antibiotics. Antibiotic and dosage prescribed depends on your condition.
Oxygen Therapy & Pulmonary Rehabilitation
Oxygen therapy – if your blood oxygen level is low or you have chronic respiratory failure characterized by fatigue, fainting and breathlessness on mild exertion, your doctor may prescribe you supplemental oxygen. In addition, you will benefit from oxygen therapy if you have sleep apnea, heart problems or/and shortness of breath. Depending on your health, you may be recommended to use oxygen permanently.
Pulmonary Rehabilitation – this technique represents a transdisciplinary and structured intervention used to treat patients suffering from chronic obstructive pulmonary disease (COPD). It reduces dyspnea (difficulty breathing), and improves the capacity to exercise and quality of life in general. Pulmonary rehabilitation can be performed by various specialists such as doctor, physiotherapist, nutritionist or psychologist.
Usually, a pulmonary rehabilitation is a combination of exercise training, and nutritional, educational and psychosocial support. Exercise training is an essential element of any pulmonary rehabilitation program. It is based on supervised sessions of 30 to 45 minutes of exercise at high intensity, 3 to 5 times per week for at least 20 sessions.
Surgical treatment
In case the other alternatives do not work or complications, surgery will be the only option to control your COPD symptoms. Usually, your surgeon will perform either lung volume reduction surgery or lung transplantation.
Lung Volume Reduction Surgery (LVRS) – LVRS is an innovative surgical treatment reserved for patients with severe emphysema, one of several respiratory disorders labeled as chronic obstructive pulmonary disease (COPD). During the surgery, the damaged part of the lung is removed, which allows the healthy remaining tissue to expand and work better.
Lung transplant – this is a surgical procedure used in patients who can’t breathe without additional oxygen, or who have severe lung damage. During the procedure, the surgeon removes the diseased lung and replaces it by a healthy one, which can be from a dead or a living person. A lung transplant should be the last step in the treatment of COPD; it has many complications, and success is not fully guarantee.
COPD Prevention
If you want to prevent COPD do not smoke. If you are already a smoker, stop smoking; this is the best preventive method. Because effects of cigarette can last years after you stop, earlier you quit better chance you have to live a life free of COPD and a variety of cancers.
In addition, you need to avoid working in places that put you at greater risk of chronic obstructive pulmonary disease:
- coal mine
- hard rock mine
- tunnel
- concrete Industry
- rubber manufacturer
- leather
- public utilities
- textile
- Construction or other occupations that expose you to cigarette smoke, polluted air and various gases, dusts and fumes.
References:
1 – WHO Media centre, Bronchopneumopathie chronique obstructive (BPCO): Aide-mémoire N°315
Mai 2008
2 – MedlinePlus Medical Encyclopedia: Chronic obstructive pulmonary disease
3 – MedicineNet.com – COPD signs & symptoms
4 – MedicineNet.com – COPD causes
5 – Løkke A, Lange P, Scharling H, Fabricius P, Vestbo J (2006). “Developing COPD: a 25 year follow up study of the general population”. Thorax 61 (11): 935–9. doi:10.1136/thx.2006.062802. PMID 17071833.
6 – Devereux, Graham (May 2006). “ABC of chronic obstructive pulmonary disease. Definition, epidemiology, and risk factors“. BMJ 332 (7550): 1142–4. doi:10.1136/bmj.332.7550.1142. PMID 16690673.
7 – Hnizdo E, Vallyathan V (April 2003). “Chronic obstructive pulmonary disease due to occupational exposure to silica dust: a review of epidemiological and pathological evidence“. Occup Environ Med 60 (4): 237–43. doi:10.1136/oem.60.4.237. PMID 12660371.
8 – mayoclinic.com, COPD Symptoms
9 – mayoclinic.com, test and diagnosis
10 – Culture des expectorations: Soins infirmiers en médecine et en chirurgie: 2. Fonctions respiratoire … Par Lillian Sholtis Brunner, Suzanne C. Smeltzer, Brenda Bare,
11- Gaz du sang (GDS), Sante.public.lu
12 – nyp.org, New York-Presbyterian Hospital; Lung Volume Reduction Surgery
13 – sciencedirect.com, La Presse Médicale Volume 38, Issue 3, March 2009, Pages 452-461: Bronchopneumopathie chronique obstructive
14- http://www.thefreedictionary.com/phlegm
15 – Conese, M; Piro, D; Carbone, A; Castellani, S; Di Gioia, S (2014). “Hematopoietic and mesenchymal stem cells for the treatment of chronic respiratory diseases: role of plasticity and heterogeneity.”. TheScientificWorldJournal 2014: 859817. doi:10.1155/2014/859817. PMC 3916026. PMID 24563
16 – An outcomes strategy for people with chronic obstructive pulmonary disease (COPD) and asthma in England (PDF). Department of Health. 18 July 2011. p. 5. Retrieved 27 November 2013.
17 – Bloom, D (2011). The Global Economic Burden of Noncommunicable Diseases (PDF). World Economic Forum. p. 24.
18 – Nici, Linda (2011). Chronic Obstructive Pulmonary Disease: Co-Morbidities and Systemic Consequences. Springer. p. 78. ISBN 978-1-60761-673-3
19 – Wright, Joanne L.; Churg, Andrew (2008). “Pathologic Features of Chronic Obstructive Pulmonary Disease: Diagnostic Criteria and Differential Diagnosis” (PDF). In Fishman, Alfred; Elias, Jack; Fishman, Jay; Grippi, Michael; Senior, Robert; Pack, Allan. Fishman’s Pulmonary Diseases and Disorders (4th ed.). New York: McGraw-Hill. pp. 693–705. ISBN 978-0-07-164109-8.
20 – Jindal, Surinder K (2013). Chronic Obstructive Pulmonary Disease. Jaypee Brothers Medical. p. 139. ISBN 978-93-5090-353-7
21 – Chapman, Stephen (2009). Oxford handbook of respiratory medicine (2nd ed.). Oxford: Oxford University Press. p. 707. ISBN 978-0-19-954516-2.
22 – Blackler, Laura (2007). Managing chronic obstructive pulmonary disease. Chichester, England: John Wiley & Sons. p. 49. ISBN 978-0-470-51798-7
23 – Gartlehner G, Hansen RA, Carson SS, Lohr KN (2006). “Efficacy and Safety of Inhaled Corticosteroids in Patients With COPD: A Systematic Review and Meta-Analysis of Health Outcomes”. Ann Fam Med 4 (3): 253–62. doi:10.1370/afm.517. PMC 1479432. PMID 16735528
24 – Decramer ML, Hanania NA, Lötvall JO, Yawn BP (2013). “The safety of long-acting β2-agonists in the treatment of stable chronic obstructive pulmonary disease”. Int J Chron Obstruct Pulmon Dis 8: 53–64. doi:10.2147/COPD.S39018. PMC 3558319. PMID 23378756
25 – Liesker JJ, Wijkstra PJ, Ten Hacken NH, Koëter GH, Postma DS, Kerstjens HA (February 2002). “A systematic review of the effects of bronchodilators on exercise capacity in patients with COPD”. Chest 121 (2): 597–608. doi:10.1378/chest.121.2.597. PMID 11834677
26 – Vestbo, Jørgen (2013). “Introduction”. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (PDF). Global Initiative for Chronic Obstructive Lung Disease. xiii–xv.
27 – Policy Recommendations for Smoking Cessation and Treatment of Tobacco Dependence. World Health Organization. pp. 15–40. ISBN 978-92-4-156240-9